
 Added to basket
Added to basket

 Unapplied Changes
Unapplied Changes








































The Non-Surgical Rhinoplasty (NSR) is a treatment very close to my heart as, for as long as I can remember, I have always been unhappy with the appearance of my nose. In 2016, I was due to undergo surgery to have the dorsal hump corrected. After completing my initial NSR course I opted for this treatment myself, cancelled my surgery and I have never looked back! It literally transforms a person’s face and, with it, the confidence they ooze. With lots of benefits that prevail on surgery which I will list below. I find it the most rewarding treatment to deliver and I am yet to experience an unsatisfied patient. The results are instant, and the downtime is minimal.
The basics
The procedure is non-invasive, taking around 10-15 minutes of injecting time to complete and therefore, much more affordable. Though some patients will experience undesirable yet common side effects i.e., bruising/swelling, the risk involved is also much lower than that of a surgical rhinoplasty.
In addition, NSR allows the practitioner to sculpt, mould or build/add volume to the nose, which is why natural and subtle results can be delivered as opposed to a drastic change. In my personal and professional opinion, it can really transform an individual’s confidence.
Anatomy of the nose
When injecting a nose, it is important to view the face holistically, taking into account other facial features that may help to balance the profile and harmonise the face—particularly when a patient feels their nose is “too big” for their face. This is often due to a lack of proportion and balance in the profile i.e., projection of the pogonion, lips and forehead. On occasions, to improve a patient's nose they may need treatments alongside the non-surgical rhinoplasty such as chin augmentation and lip enhancement.
Any practitioner carrying out a NSR must have a sound knowledge of the anatomical structures that create the nose. They must understand their function and respect each person’s anatomy on an individual basis, as we are not all text book.
The nose is mostly constructed of bone and cartilage. Aesthetic nose complaints are often due to the vast variations in cartilage amongst patients; it is important to note that these variations can contribute to the differences in anatomical structures i.e., placement of arteries from individual to individual. We take particular caution when treating a nose that has undergone corrective surgery or has previously been broken, as we know from various research papers that these factors affect the anatomy.
Nasal Muscles
We are mindful of the muscle structures in the nose and their elevating and depressing functions. The nasalis is the largest muscle covering the nose and is responsible for nasal flaring. We assess the extent of nasal flaring with every patient and from time to time it is necessary to treat this muscle with a toxin to reduce the flaring and the size of the nostrils.
The depressor septi-nasi is responsible for the drop of the tip. The more active this muscle is, the larger the droop. In some instances, a combined approach to treatment is required using botulinum toxin to reduce the muscle function and later treating with HA Dermal Filler to provide a support for the tip elevation.
Blood Supply
The facial artery, branching off into the angular artery, is responsible for the majority of the blood supply to the nose; branching from these are the dorsal artery, lateral nasal artery and septal branch. These nasal arteries are end arteries, meaning they are the sole supply of oxygenated blood to that part of the face. There is very little space between bone and skin, and these vessels are all encased in this tight space, therefore when injecting this area, it is of particular risk.
The dorsal artery is connected to the ophthalmic artery and there has been reported incidents of eyesight loss from vascular occlusions that have occurred in the nose following treatment with HA dermal filler. You must be aware of the depths of the arteries within the nose. We always inject to bone in the upper aspect of the nose, however towards the tip of the nose, our injection placement is shallow, as we do not want to widen the cartilage plates and the gathering of vessels in the nasal tip are located deep within the tissue. It is still possible to cause a vascular compromise however, so we advocate aspiration on each injection along with thorough assessment of the capillary refill, tone and temperature of the injection site and surrounding tissue.
Skin
The skin towards the top of the nose is fairly thin in comparison to that in the lower nose, and again we bare this in mind when injecting. If dermal filler is placed too superficially in the nasofrontal angle, it is not uncommon for the patient to experience filler migration laterally on the nose.
What is your recommended injection plan?
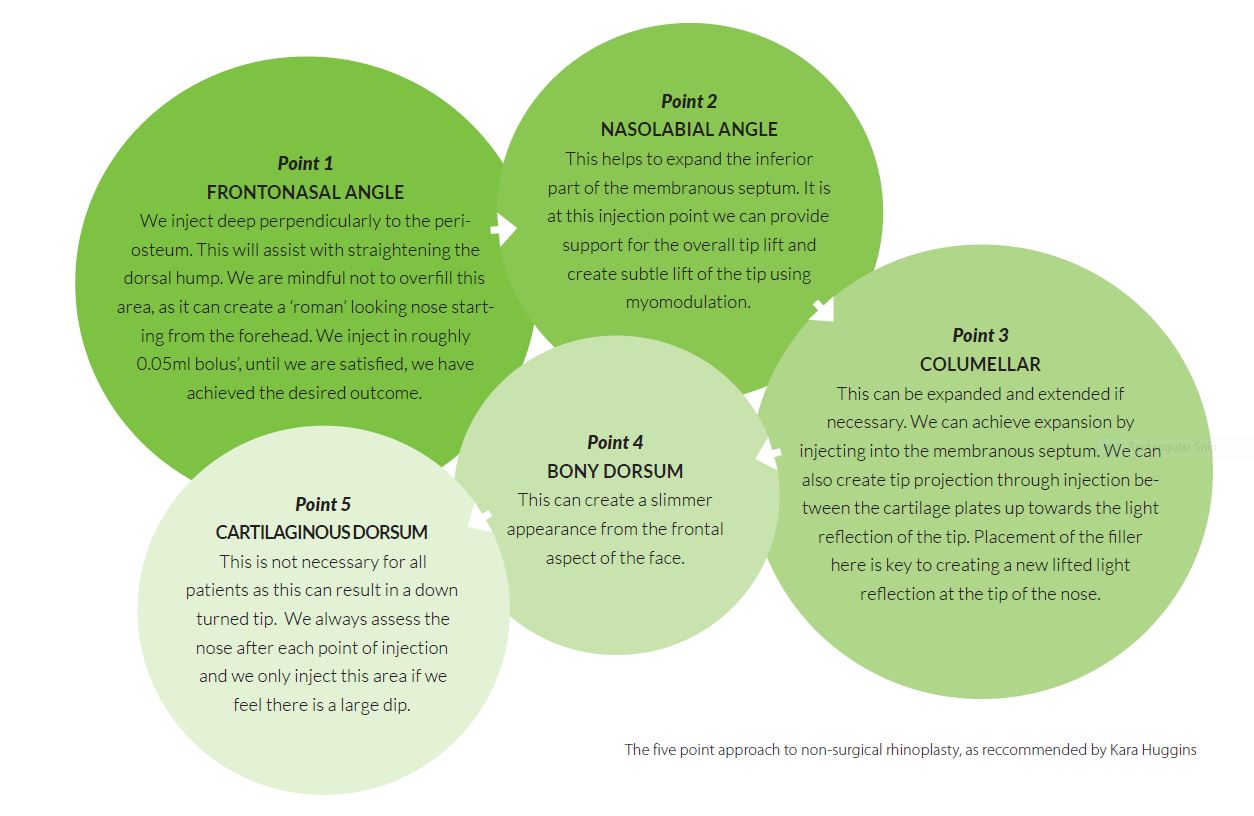
We recommend a five-point approach to NSR. When assessing the nose, it is important to take into consideration other landmarks i.e., the projection of the chin, forehead and lips, as well as the angles:
Nasolabial norms: Male 90-95°. Female 100-105°. The tip rotation should be observed when assessing this landmark.
Nasofrontal norms: 120-130° male, 115-125 females
Columellar show: 3-5mm on show, although in some ethnic origins this is not on show at all. By lifting the tip, we can create the illusion of a columellar show.
It is useful to spend at least 15 minutes during a consultation assessing these landmarks and angles, and discussing these in depth with your patient. It is a great opportunity for profile analysis and to manage expectations. We recommend assessing the nose in relation to the face from all angles (front facing, profile, 45-degrees and so forth) to properly assess light reflection. We would also assess this on expression and when the patient remains static.
Prior to treatment, we apply a topical anaesthetic. This makes the procedure a little more comfortable and tolerable for our patients. Once this has been removed, we thoroughly assess the skin and anatomy in the area we are to treat. Palpating for vessels, documenting capillary refill times and assessing skin colour and temperature ‘to touch’ – this provides a great baseline for comparison post treatment and allows us to quickly identify any vessel compromise or complications.
Needle or cannula?
Our preferred method of injection in our clinic is with a needle, as in our experience we find it is more comfortable than a cannula for the patient and we can be more precise with our injection location. Overall, we find injecting with a needle gives more satisfactory results. However, we would from time to time use a cannula if treating a patient who had undergone corrective surgery previously or had broken their nose, due to the potential altered anatomy this presents with. In our opinion, a cannula provides an added safety net.
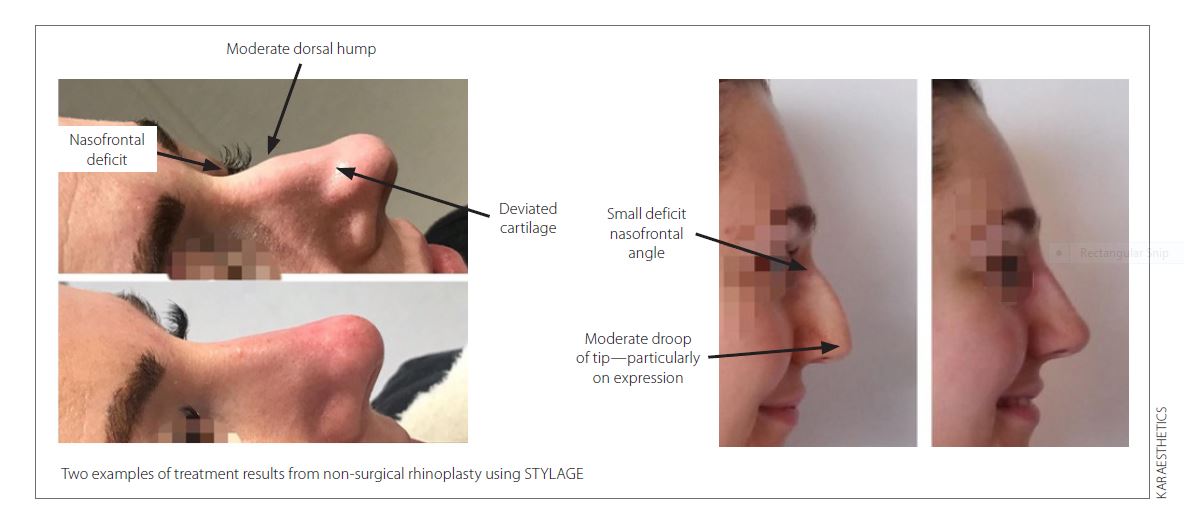
Our preferred product for the non-surgical rhinoplasty is STYLAGE XL or XXL, due to their ability to maintain structure and the longevity of the product. However, if using a cannula, we find the pressure required to deposit the filler can cause added discomfort to the patients' experience. Opting for STYLAGE L in this case will still give outstanding results in our professional opinion.
The most amount of HA filler we will deposit during a NSR is 1ml, however it is rare that this amount of product is required, and often we use between 0.3ml and 0.6ml to complete a NSR.
What are the potential complications, and how can you avoid them?
The most frightening complications faced by any patient undergoing an NSR or practitioner undertaking an NSR is of course a vascular occlusion (VO). This can lead to eyesight loss and tissue necrosis if left unidentified and untreated.
We would always advise you gain a baseline assessment of the patient’s facial tissue prior to injecting. One huge mistake we find is often made is the lack of thorough assessment of the capillary refill. We recommend this is assessed by applying firm pressure to the tissue for a minimum of 5 seconds before releasing the pressure and measuring the amount of time it takes for the blood flow to return. Due to the nature of the arteries in our face we will always record the capillary refill in the nasal area, both medially and laterally, the nasal tip, the forehead and the lips and chin. As potentially a vessel blockage in the nose can cause compromisation of blood flow anywhere in these aforementioned areas.
We also recommend a subtle and conservative approach to injecting a nose. Administering small boluses of no more than 0.05ml at a time, moulding and assessing the tissue after every injection. This will also help to make any vascular compromise much more manageable.
We often perform NSRs in two sittings, as we find the initial result can settle and small deficits can return once the internal swelling has dispersed and the healing process is underway.
We also find that some practitioners will confuse a VO with bruising. Blood supply may be compromised if a patient experiences a drastic haematoma or bruise due to the internally swelling and leakage of blood in the surrounding tissue. However, this is very different to that of a VO.
Treating VO
We perform roughly 15-25 NSRs per week and we have in fact experienced a VO in the nose only last year. This was identified within minutes and through thorough assessment we could locate roughly where the occlusion had occurred, which was in fact in the nasofrontal angle. We applied heat and vigorous massage and followed our clinic protocol for emergency treatment and we used 6000iu hyaluronidase to dissolve the filler. The patient remained with us in clinic for five hours and was reviewed the next morning at 8am. We discuss this case in detail during our training courses with our delegates, as it provides a great learning opportunity.
Other complications include haematomas, if we encounter a large haematoma (which is uncommon but happens) we will cease injecting and invite the patient back to clinic two weeks later to complete the treatment.
Kara Huggins is the founder of KarAesthetics in Hull, an Advanced Aesthetics Nurse Practioner and Lead Trainer.
Recommended further reading
Bouaoud, J. Belloc, JB_ Use of injectables in rhinoplasty retouching: Towards an evolution of surgical strategy? Literature review. Journal of Stomatology, Oral and Maxillofacial Surgery. 2020; 121(5): 550-555.
Stevens, MR. Emam, HA. _ Applied Surgical Anatomy of the Nose. Oral and Maxillofacial Surgery Clinics of North America. 2012; 24(1): 25-38.
